4 Vetrano DL (2018)
Saturday Morning RStudio 勉強会
毎週土曜朝6:30-9:00
4.1 論文
それでは、実際にメタ分析を扱っている論文を見てみましょう。British Medical Journal のオープンアクセス版である BMJ Open に掲載されています。
Corresponding author は Dr Graziano Onde です。このサイトでは、ORCID などにはリンクしていないようです。
Vetrano DL, Palmer KM, Galluzzo L, Giampaoli S, Marengoni A, Bernabei R, & Onder G (2018). Hypertension and frailty: a systematic review and meta-analysis. BMJ open, 8(12), e024406.
http://dx.doi.org/10.1136/bmjopen-2018-024406
Creative Commons Attribution Non Commercial (CC BY-NC 4.0)
この論文では、フレイル患者の高血圧有病率とオッズ比をプールしています。
著者は、第一著者は Davide L Vetrano で、所属 (affiliation) は二つあります。一つはスェーデンのカロリンスカ研究所で、もう一つはイタリアの大学です。他の著者も見てみると、どうやらイタリアの研究者のようです。1
1 What is the affiliation of the corresponding author?
4.2 Abstract
まずは Abstract を読んでみましょう。
Objective To review the association between hypertension and frailty in observational studies.
観察研究において、高血圧とフレイルの関連をレビューすることが目的です。
Design A systematic review of the PubMed, Web of Science and Embase databases was performed. A meta-analysis was performed if at least three studies used the same definition of frailty and a dichotomous definition of hypertension.
系統レビューに用いたデータベースは3つです。フレイルの定義方法が同じであり、高血圧を有無で報告している研究が3つ以上ある場合、メタ分析をしています。2
2 What is the study design?
dichotomous: 二値変数。binary ともいう。ここでは「高血圧あり」と「高血圧なし」の2値と思われます。
Setting, participants and measures Studies providing information on the association between frailty and hypertension in adult persons, regardless of the study setting, study design or definition of hypertension and frailty were included.
高齢者のフレイルと高血圧の関係についての研究を含めた、とあります。研究デザイン、高血圧やフレイルの定義は指定していません。
多くのメタ分析では、「ランダム化比較試験だけ」や「Fried 基準のフレイルだけ」というように、条件を狭めた上で系統レビューすることがあります。この研究では広めに検索したようです。
Results Among the initial 964 articles identified, 27 were included in the review.
メタ分析に先立つ系統レビューでは、まず検索結果について報告します。最初に 964 件の研究がヒットし、組入基準や除外基準を適用して 27 件に絞りました。3
3 How many studies were included for the review?
ここで気になる点があります。最初に 1000 件近くあったのに、最終的に 30 件未満になってしまい、組み入れられたのは 3% 以下です。こんなに少なくて良いのでしょうか?実際、多くの系統レビューでは、組み入れられる件数はこの程度のようです。
Four longitudinal studies examined the incidence of frailty according to baseline hypertension status, providing conflicting results.
4 件の縦断研究が、ベースライン時点で高血圧にある人が、その後にフレイルを発症したことを検証しました。しかし、研究間で一致していないようです。どう一致していないかは、本文を読む必要がありそうです。
縦断研究とは、2 回以上調査を行ったという意味です。なお、縦断の反対は「横断」 (cross-sectional) で、1回限りの調査です。
incidence: 「発症」や「発生」などの意味です。incident dementia は「認知症発症」、incident hospitalisation は「(初めての) 入院の発生」というような使い方をします。 医療現場では、「インシデント」というとアクシデントの手前という意味もありますが、ここではちょっと違う意味です。
つまり、ベースラインでは全員「フレイルなし」な状態で、一部の人は高血圧ありということになります。その後にフレイルを発症した人数について「高血圧あり群」と「高血圧なし群」に有意差があるかどうかを調査したことになります。
Twenty-three studies assessed the cross-sectional association between frailty and hypertension: 13 of them reported a significantly higher prevalence of frailty in hypertensive participants and 10 found no significant association.
英語では、数字は 1 桁の数字はアラビア数字を使わず、英語でスペルアウトします。また、文の最初もスペルアウトすることが多いです。
23 件は横断研究で、フレイルと高血圧の関係を調べました。こちらは時間的な差がない研究で、13 件は高血圧とフレイルには関連あり、10 件は関連ありとは言えないとなっています。
The pooled prevalence of hypertension in frail individuals was 72% (95% CI 66% to 79%) and the pooled prevalence of frailty in individuals with hypertension was 14% (95% CI 12% to 17%).
これは、前の 23 件についてだと思われます。メタ分析によってプールした結果、フレイルの人の 72% が高血圧でした。また、高血圧の人の 14% がフレイルでした。4
4 What is the pooled prevalence of hypertension in individulateds with frailty?
individual/person/patient with 病名: 〜病患者
カッコの中には、 95% CI という語があります。CI は Confidence Interval の略語ですが、定義せずに使っています。Abstract 中で定義せずに使われるほど、「誰でも知っている略語」という扱いになっています。
Five studies, including a total of 7656 participants, reported estimates for the association between frailty and hypertension (pooled OR 1.33; 95% CI 0.94 to 1.89).
結果の最後は、フレイルと高血圧の関連を調査した 5 件の結果をプールしたもので、オッズ比が 1.33 となりました。ただし、95 % CI が 1 を含んでいるため、有意差があるかどうかはわかりません。
Conclusions Frailty is common in persons with hypertension. Given the possible influence of frailty on the risk–benefit ratio of treatment for hypertension and its high prevalence, it is important to assess the presence of this condition in persons with hypertension.
結論では、高血圧の人にフレイルはよくあると述べていますが、これは 14% という結果からあまり強くは言えないのではないでしょうか。この逆の「フレイルの人には高血圧が多い」とは言えそうです。結論としては、高齢者は高血圧もフレイルもどちらも注意すべきという一般的な示唆となりました。
4.3 Introduction
Introduction の第 1 段落は、フレイルについての基本事項から始まります。
Frailty is a condition characterised by the accumulation of biological deficits and dysfunctions which occurs with age and impairs the homeostatic balance of organisms.\(^1\) Frailty confers extreme vulnerability to stressors and increases the risk of negative health outcomes, including mortality, disability, poor quality of life, hospitalisation and institutionalisation.\(^2\) This condition has a high prevalence, ranging from 8% to 16% in community-dwelling older adults.\(^{3 4}\) Frailty has been shown to be correlated with morbidity and mortality in persons suffering from cardiovascular disease, and it was suggested that the recognition of frailty status can help physicians in establishing prognosis, determining procedural risks and guiding treatments.\(^5\) In some cases, the assessment of frailty may be critical in guiding the patient towards a certain therapeutic choice.\(^6\)
第一文を読んでみましょう。
Frailty is a condition 1{characterised by the accumulation of biological deficits and dysfunctions} 2{which occurs with age and impairs the homeostatic balance of organisms}.\(^1\)
characterised by the accumulation of biological deficits and dysfunctions と which occurs with age and impairs the homeostatic balance of organisms は、どちらも a condition にかかります。
フレイルとは、1{生物学的欠損と機能障害の集積によって特徴づけられ}て2{年齢とともに発生し組織の恒常性バランスを害する}ような状態である。
文の後の上付き数字 1 は、引用文献を示しています。これは、Discussion よりも後に書かれています。
- World Health Organization. World report on ageing and health. Geneva, Switzerland: World Health Organization, 2015.
このように、引用文献がある場合は、筆者の意見というよりも引用文献の意見になります。第1段落は、すべて引用がついています。フレイルについての現在の知見を簡潔にまとめたものになっています。5
5 フレイルが、循環器疾患患者の死亡に関連しているとする引用文献はどれか?
第2段落に移りましょう。高血圧について触れいています。
Several studies have assessed the association of frailty with hypertension. In older adults, it has been suggested that frailty can explain the paradoxical relationship between lower blood pressure (BP) and increased mortality documented in several studies.\(^{7–10}\) For example, data from the National Health and Nutrition Examination Survey demonstrated an effect modification of hypertension according to frailty level in terms of walking speed\(^{11}\) ; in fit persons, elevated BP was associated with greater mortality, while in frail participants higher BP was associated with lower mortality risk. The SPRINT trial showed that compared with standard BP control intensive control reduces the incidence of cardiovascular events both in frail and non-frail persons, but this study did not show any effects of intensive BP control on risk of frailty-related outcomes, such as gait speed and mobility limitation.\(^{12 13}\) Notably, the hypertension clinical practice guidelines released in 2017 precisely point out that BP-lowering therapy is one of the few interventions shown to reduce mortality risk in frail older individuals.\(^{14}\)
in fit persons, elevated BP was associated with greater mortality, while in frail participants higher BP was associated with lower mortality risk.
fit: 「健康な」の意味。辞書によっては、She is fit. のような叙述用法しか使われないと指摘しているものがあるが、ここのように限定用法でも用いられる。
elevetd BP: 直訳すると「上げられた血圧」となるが、「血圧の上昇」と訳す。
健康な人の場合、血圧の上昇は死亡率の上昇と関連があるが、フレイル参加者は高血圧と死亡率減少が関連する、とあります。
最終段落に移ります。
Assessing the association of frailty and hypertension may be the first step for understanding their complex interplay and might ultimately lead to optimise the treatment of hypertension and to set therapeutic goals in persons with frailty. However, the evidence on the association between these conditions has never been comprehensively summarised. The aim of the present study is to systematically review the literature and provide pooled estimations of evidence regarding the association of frailty and hypertension.
フレイルと高血圧の関連について、まだ証拠が十分ではないので、この研究でレビューします。6
6 What is the purpose of this study?
4.4 Methods
方法論に移ります。
We reviewed studies providing information on the association between frailty and hypertension in adult persons (ie, 18 years or older), regardless of the study setting, study design or definition of hypertension and frailty. The protocol of the present study was registered in the international prospective register of systematic reviews (registration number CRD42017058303). This systematic review was carried out in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses recommendations.
We reviewed studies providing information on the association between frailty and hypertension in adult persons (ie, 18 years or older), regardless of the study setting, study design or definition of hypertension and frailty. …
ここでは、成人のフレイルと高血圧の文献をレビューしています。高齢者に限ってはいないようですね。
regardless: 〜にもかかわらず、〜を考えないで
ここでは、後者の方がわかりやすいと思います。
研究のセッティング、研究デザイン、高血圧やフレイルの定義を考えない、というよりも、これらについて除外基準を設けていないということです。
多くのメタ分析では、例えば「フレイルの定義として Fried 基準を使っているものだけ」などのように組入・除外基準を設けています。この論文はそうではないということです。
このほか、事前に登録していることと、報告にあたって PRISMA に従っていることを示しています。
登録は、こちらで確認することができます。7
7 サイトを開き、登録番号を検索して現在の状態を確認してみよう。
https://www.crd.york.ac.uk/prospero/
Data sources and searching
We searched three databases for relevant articles published from 1 January 2002 to 26 October 2017: (1) PubMed electronic database of the National Library of Medicine, (2) Web of Science and (3) Embase. The detailed search queries are reported in the online supplementary appendix. References from the selected papers and from other relevant articles were screened for potential additional studies.
ここでは、検索に用いたデータベースを示しています。
臨床研究では、MEDLINE (PubMed) や Embase が良く用いられます。ここでは、これに加えて Web of Science も利用しています。
Study selection and data extraction
Two assessors independently screened the title and abstract of the selected studies. The inclusion criteria were (1) articles reporting information on the association of frailty with hypertension or BP values; (2) articles in English or another European language; and (3) study design: cross-sectional, case–control or cohort studies. Articles were excluded if they (1) did not investigate the aims of the review; (2) included persons younger than 18 years; (3) did not report original data (eg, editorial, review or congress abstract); (4) did not provide an explicit definition of frailty; (5) if frailty was assessed only with a single symptom/measure (eg, only gait speed or grip strength) and (6) were not in English or another European language. The full text of the articles selected by one or both of the assessors was retrieved for full evaluation. Two assessors read the full texts and independently extracted the information from the selected studies. A third assessor reviewed the data extraction, and any disagreement was resolved through consensus. Articles that were written in another European language than English were sent for translation by a native speaker who conducted the data extraction.
この段落では、検索に用いた条件を述べています。8
8 英語以外の論文はすべて除外されたか?
近年では、実際に検索に使ったキーワードを記すことも多いのですが、ここでは記されていません。
… Two assessors read the full texts and independently extracted the information from the selected studies. …
2人の評価者が論文を読み、独立して情報を抽出しました。
組入基準と除外基準が書かれています。
Assessment of risk of bias
Quality of the studies was evaluated independently by the two assessors with the qualitative evaluation of observational studies Newcastle Ottawa Scale (NOS). Any disagreement in quality assessment was resolved through consensus. Studies scoring >7 were considered at low risk of bias, scores of 5–7 indicated moderate risk of bias and scores of <5 indicated high risk of bias.
研究の質については、バイアスのリスク (risk of bias) という評価方法があります。
ここでは、NOS をいう評価手法を用いました。これは、最大 9 項目の評価手法です。9
9 バイアスリスクが低いとするのは NOS 何点か?
Statistical analysis
For each measure of interest (ie, proportions and association estimates), a meta-analysis was performed if at least three studies used the same definition of frailty and a dichotomous definition of hypertension (rather than using continuous BP values). Considering the observational design of the retrieved studies, and the methodological differences potentially responsible for a significant share of the variance within the measures of interest, the pooled estimates were obtained through random-effect models and Mantel-Haenszel weighting. Lack of homogeneity within the pooled studies was tested through the I\(^2\) statistics (significant if ≥50%). Additional analyses were performed selecting (1) studies with NOS ≥5 in order to exclude studies with high risk of methodological bias and (2) studies with a sample size ≥500 participants. Publication bias was assessed by mean of the Egger’s and the Begg’s tests. All statistical analyses were performed using the metan and metaprop packages included in STATA V.14.0. Metan was used to provide pooled estimations of the association between frailty and hypertension, Metaprop was used to provide pooled measures of prevalence of frailty and hypertension.\(^{15 16}\) A p value <0.05 was considered statistically significant for all analyses.
… a meta-analysis was performed if at least three studies used the same definition of frailty and a dichotomous definition of hypertension (rather than using continuous BP values).
同じフレイル定義を用い、高血圧は二値変数を用いている研究が 3 以上ある場合にメタ分析を行いました。
homogeneity: 同質性
血圧は、そのまま数値と用いることももちろん可能ですが、カットオフ値を設定して高血圧とそうでないという二値変数で扱うこともあります。ここでは後者を使いました。
Patient and public involvement
Patients and public were not involved in this study.
これは、ある意味当然ですね。系統レビューとメタ分析は、すでに出版された論文等を再解析するものです。実験参加者はいません。
4.5 Results
結果に入ります。
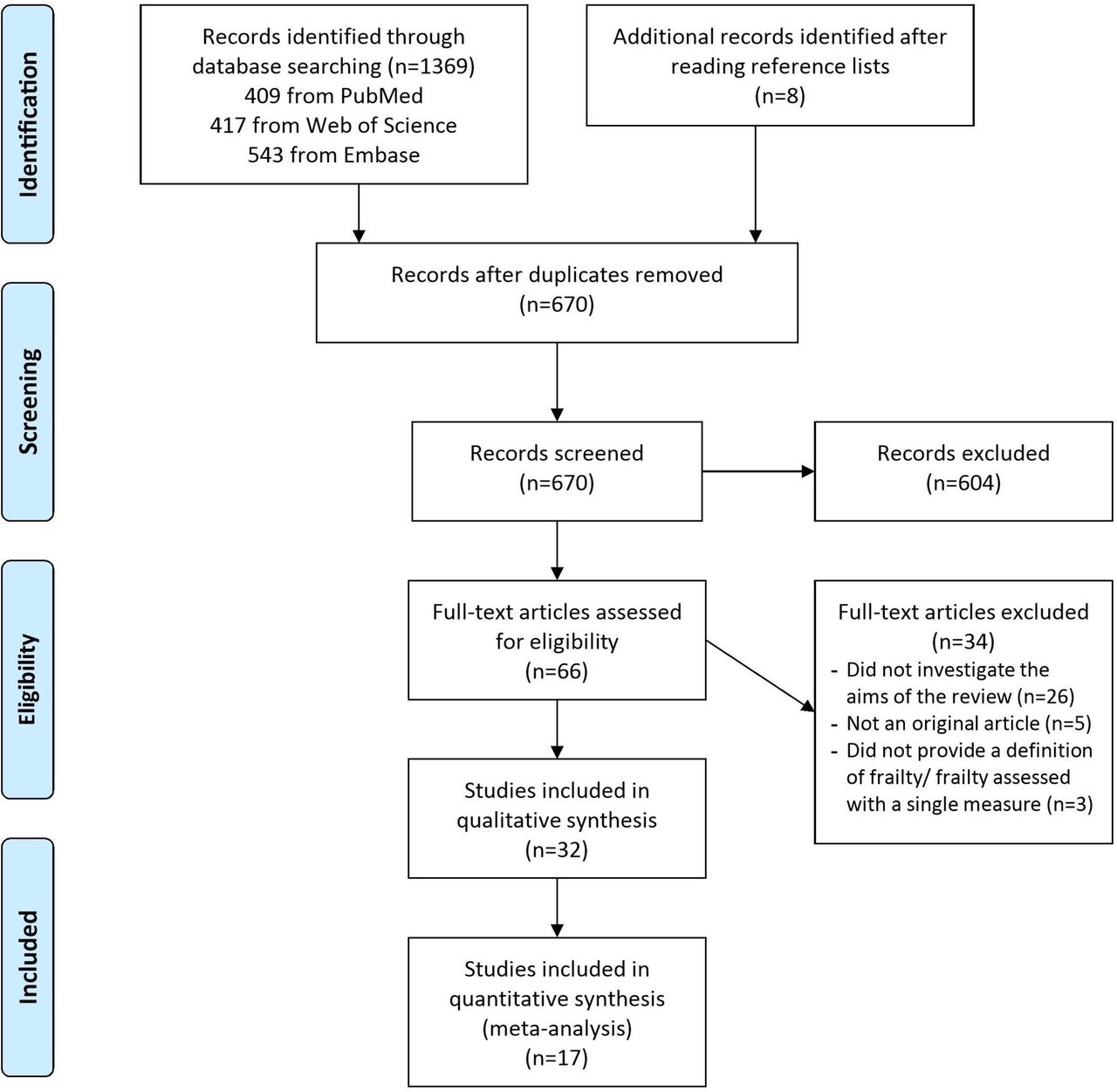
Through the literature search, we retrieved 1369 articles (figure 1). An additional eight articles were identified after reading references from the selected papers. Out of 1369 articles, 670 (48.9%) were screened after duplicates removal. Of these, 604 were excluded after screening and 34 after full-text reading. Thirty-two articles were part of the final qualitative and/or quantitative assessment\(^{17–48}\) (see table e1 in the online supplementary appendix).
系統レビューでは、まず検索の件数を報告します。ここでは、3つのデータベースで 1369 件とその他 8 件見つかり、重複を除外すると 670 件残りました。
Of these, 604 were excluded after screening …
次に、604 件が除外されたとあります。ここでは書かれていませんが、おそらくタイトルと Abstract から判断されたのでしょう。これで、残りは 66 件です。10
10 フルテキストを読んだ件数は何件か?
質的合成には 32 件、その中からさらにメタ分析は 17 件が選ばれました。
以上をまとめた物が Fig 1 になります。
Study description
The studies’ sample size ranged from 56 to 144 403 participants, with a mean age ranging from 60 to 81 years. Only four studies had a longitudinal design.\(^{17–20}\) Most studies included community-dwelling participants, and only three studies included in-hospital participants.\(^{43 47 48}\) Most of the studies were carried out in Asia (n=10), Europe (n=9) and South America (n=9), and fewer in North America (n=4).
サンプルサイズが 56 から 144,403 を大きく異なっています。ただし、これが 質的研究もふくめてなのか、メタ分析に欠けている 17 件のことなのかが、はっきりしません。この点は、Figure 1 と関連してきますので、覚えておきましょう。
Frailty and hypertension definitions
Most of the studies (n=23) defined frailty according to the Cardiovascular Health Study (CHS) criteria.\(^{17–19 21 22 24 25 27–30 34 36–39 41–47}\) The rest of the studies evaluated frailty based on a frailty index (n=6),\(^{20 23 26 32 38 40}\) by a composite score (n=3)\(^{31 33 35}\) or using the Clinical Frailty Scale (n=1).\(^{48}\) One study assessed frailty adopting both CHS criteria and Frailty Index (FI).\(^{38}\)
ここで n = 23 (> 17) という数値が出てきたので、今のところは質的合成のようです。23件は、定義が CHS (Fried 基準のこと) でした。11
11 フレイルの定義として、Fried LP による CHS 基準以外に何があったか?
In the longitudinal studies, frailty incidence ranged from 3% to 16%, in cross-sectional studies, and frailty prevalence ranged from 3% to 68%. A diagnosis of hypertension was reported in 28 studies,\(^{17–23 25–38 41–47}\) while three studies analysed BP as a continuous variable\(^{24 38 48}\) and one classified BP in four groups.\(^{40}\) Diagnosis of hypertension was based on a BP cut-point in 12 studies,\(^{17 18 22 28 29 31–34 36 39 41}\) assessed only by self-reported in 5 studies,\(^{21 25 43 45 46}\) based on evaluation of medical records in 1 study\(^{35}\) and on pharmacological treatment in 1 study.\(^{21}\) In nine studies, hypertension diagnosis was not defined.\(^{19 20 26 27 30 37 42 44 47}\) Prevalence of hypertension ranged from 28% to 100%.
次に、縦断研究 (longitudinal study) についてです。縦断研究とは、介入研究のように介入前後を比較したり、コホート研究で一定期間追跡調査を行うことです。
frailty incidence とは、縦断研究の追跡でフレイルが発症したことを指します。追跡期間にもよりますが、発症が3% から 16% もあったようです。
frailty prevalence は、横断研究において、フレイルの有病率を調査したものです。縦断研究においても、ベースライン時点でのフレイルの有病率を報告していることもありますが、ここでは横断研究のみ見ているようです。
高血圧の定義についてもここで書かれています。なんと、9件もの研究で高血圧の定義が書かれていなかったようです。
Assessment of risk of bias
The majority of the studies presented a moderate risk of bias (n=25), and six studies presented a high risk, according to the NOS. In most of the cases, the self-reported nature of information was responsible for a lower score. However, according to the Egger’s and the Begg’s tests, no strong evidence of publication bias was detected in our meta-analyses (p=0.150 and 0.987, respectively).
メタ分析において、研究の内的妥当性 (internal validity) のことをリスクオブバイアス (risk of bias, rob) と言います。研究者が、あらかじめ決められた評価基準に照らし、各論文を読んで評価を行います。詳細は、R によるメタ分析:ハンズオン をご覧ください。
リスクオブバイアスは、あまり良くはないようですが、かといってバイアスの証拠もないようです。
Association between hypertension and frailty
Longitudinal studies
Four longitudinal studies examined the risk of incidence of frailty according to baseline hypertension status. Two studies found that baseline hypertension did not significantly predict incidence of frailty,\({17 20}\) but Boullion et al found that hypertension was associated with an increased incidence of the combined outcome prefrailty/frailty (p=0.009).\(^{18}\) However, data from this study were not adjusted for possible confounders. Similarly, Castrejon Perez et al \(^{19}\) found that hypertension was associated with incident frailty at univariate analysis (HR 2.11, 95% CI 1.03 to 4.31), but this association was not confirmed in the multivariate analysis (HR 1.58, 95% CI 0.83 to 3.01).
まずは、縦断研究です。縦断研究の場合、参加者や研究ごとに期間がバラバラなので、リスク比の代わりにハザード比 (hazard ratio) というものを計算します。12
12 The interpretation of hazard ratio is similar to that of the relative risk. In Cox proportional hazards regression, the ratio is calculated to avoid needing to know the baseline hazard to model how various factors affect the hazard of an event. (Manual of Style 11th Edition p. 1042)
ここでは、ハザード比の 95% 信頼区間が 0.83 から 3.01 で、1を含んでいるため、有意差はあるかどうかは不明です。
Cross-sectional studies
Twenty-three studies assessed the cross-sectional association between frailty and hypertension.\({21 22 25–37 39 41–47}\) Results were very different across studies, with 13 studies reporting a significantly higher prevalence of frailty in hypertensive participants\({22,26–28,31,32,33,34,36,37,39,44,45}\) and 10 finding no significant association.\({21 25 29 30 35 41–43 46 47}\)
次に横断研究です。フレイルと高血圧に、関連があるとする研究が 13 件、関連があるとは言えないという研究が 10 件ありました。
Seventeen of these studies assessed frailty by the use of CHS criteria, for a total sample of 23 304 individuals.\(^{21 22 25 27 28 30 34 36 37 39 41–47}\) Analysing data from these studies, the pooled prevalence of hypertension in frail individuals was 72% (95% CI 66% to 79%; I\(^2\)=93.1%; figure 2) and the pooled prevalence of frailty in individuals with hypertension was 14% (95% CI 12% to 17%; I\(^2\)=96.2%; figure 3). When the analyses were limited to 13 studies enrolling participants with a mean age ≥70 years,\(^{21 22 25 27 30 34 36 39 41 42 45–47}\) the pooled prevalence of hypertension in frail individuals was 71% (95% CI 62% to 80%; I\(^2\)=95.4%) and the pooled prevalence of frailty in individuals with hypertension was 14% (95% CI 11% to 17%; I\(^2\)=97.0%).
この文章の下に、Figure 2 があります。Figure 2 に対応する文章は、以下のようになります。
Seventeen of these studies assessed frailty by the use of CHS criteria, for a total sample of 23 304 individuals. Analysing data from these studies, the pooled prevalence of hypertension in frail individuals was 72% (95% CI 66% to 79%; I\(^2\)=93.1%; figure 2)
Fried LP 定義でフレイルを評価したのは 17 件でした。図中の左の列には、17 件と Overall があります。これに対応しています。フレイル個人で、高血圧を持っている割合はプールしたところ 72% でした。

上の方から見ると、Avila-Funes et al. という研究は、0.71 なので 71% です。(0.66, 0.75) は、95% 信頼区間で、同様の調査したときに 95% の確率でこの範囲内にあります。中央の図の黒塗りの四角は 0.71 を示し、四角の大きさは Weight 6.62 を示しています。四角から伸びたヒゲが、95% 信頼区間を示しています。
Weight とは、他の研究との相対的な重要度になります。
プールした結果が Overall の行です。中央の赤い菱形と、その右側にある 0.72 という数値が、72% を示しています。
菱形の左端はと右端は、それぞれ (0.66, 0.79) を表し、菱形の大きさは Weight を表しています。
つまり、プールとは、
0.71 * 0.0662 + 0.49 * 0.0478 + 0.58 * 0.0588 + 0.53 * 0.0466 + 0.82 * 0.0599 + 0.86 * 0.0652 + … + 0.67 * 0.0570
という計算をしたことになります。
\(I^2\) とは、異質性の指標です。0% から 100% の値を取り、0% では異質性がないとされています。13
13 the range of I\(^2\) values is 0% to 100%, indicating no heterogeneity to high heterogeneity.
Three studies assessed BP as a continuous variable, finding conflicting results: one study showed significantly higher systolic BP (SBP) and diastolic BP (DBP) values in frail participants,\(^{24}\) while in two other studies frailty was associated with significantly lower BP values.\(^{38 48}\) A small study including only participants receiving pharmacological treatment for hypertension showed an inverse association between BP levels and frailty.\(^{23}\) Finally, a large study performed in >140 000 community-dwelling older adults aged ≥80 years classified SBP in five groups, showing that frailty was associated with lower SBP.\(^{40}\)
ここでは、血圧を「高血圧と普通血圧」に分けず、連続数値として扱った3件の研究について報告しています。さらに、2値ではなく5値に区分した研究が1つありました。
Among studies adopting the CHS definition of frailty and a dichotomous definition of hypertension, five reported estimates (ORs) for the association between frailty and hypertension, for a total sample of 7656 individuals.\(^{29 39 42 45 47}\) All five studies enrolled a sample with a mean age ≥70 years. The pooled estimate for the association of frailty and hypertension based on these studies was 1.33 (95% CI 0.94 to 1.89; I\(^2\)=79.2%; figure 4). These results were confirmed when only studies with NOS ≥5 (OR 1.39; 95% CI 0.70 to 2.75; I\(^2\)=88.1%) or studies with a sample size ≥500 participants (OR 1.25; 95% CI 0.79 to 1.99; I\(^2\)=88.4%) were analysed.
CHS 基準のフレイルと 2 値血圧を採用した研究は、5 件ありました。
その 5 件はいずれも対象者の平均年齢が 70 以上で、フレイルと高血圧のオッズ比は、95% 信頼区間が 0.94 から 1.89 であり、1 を含んでいることから、有意差があるとは言えませんsでした。
この結果は、対象を一部変更しても変わりませんでした。14
14 感度分析を行うにあたり、どのような研究に絞ってメタ分析を行なったか?
なお、対象を一部変更しても結果が変わらないかどうかを確認することを、感度分析 (sensitivity analysis) と言います。感度分析を行うことは、Methods などにも書かれておらず、唐突な印象があります。
4.6 Discussion
考察に入ります。第 1 段落は、結果の要約です。
This systematic review and meta-analysis shows that 7 out of 10 frail adults have hypertension, while about 1 out of 7 hypertensive adults present with frailty. In addition, this study shows that the association between frailty and hypertension is uncertain: few longitudinal studies have assessed the impact of hypertension on incident frailty, providing conflicting results. Further, no studies have been performed to examine whether frailty predicts incident hypertension. Finally, the meta-analysis of cross-sectional studies failed to find a significant association between these conditions.
フレイル 10 人のうち 7 人が高血圧であることがわかりました。逆に、高血圧の人 7 人のうち 1 人がフレイルでした。
しかし、フレイルと高血圧の関係ははっきりしません。
結果では「有意差はなかった」とありましたが、これだけで「関係はなかった」と結論づけられるものではありません。
incident frailty はフレイル発症、incident hypertension は高血圧発症の意味です。縦断研究 (longitudinal study) において、ベースラインで未発症であったが、追跡時点で発症していたことを指します。
「高血圧患者がフレイルを発症するかどうか」については、研究間で矛盾した結論が出ています。逆に、「フレイル患者が高血圧発症するかどうか」については、そのような研究がありませんでした。
Frailty has become a high-priority theme in cardiovascular medicine due to the ageing and the increasingly complex nature of patients suffering from cardiovascular conditions.\(^{5 6}\) This is confirmed by the observation that 14% of persons with hypertension are frail. Frailty might indeed influence the therapeutic choices for many cardiovascular diseases. For example, assessment of frailty is considered important for determining which patients are likely to benefit from the treatment of aortic stenosis or left ventricular assist device therapy, in terms of both survival and improved quality of life.\(^{49 50}\)
aortic stenosis: 大動脈弁狭窄症
left ventricular assist device: 左室補助人工心臓
Similarly, therapeutic choices in hypertension might be influenced by presence of frailty. First, frail older people are almost always excluded from randomised controlled trials (RCTs) assessing the effects of treatments of cardiovascular diseases, including hypertension. Logistic barriers limiting the retention in the study, the higher propensity to present adverse effects from the treatments and the higher drop out for mortality of frail individuals are the main causes for exclusion from RCTs.\(^{51}\) This limits the generalisability of RCTs’ findings and makes difficult estimating the efficacy and safety of treatments for chronic diseases in persons with frailty. This is extremely important if we consider that according to our results 70% of frail individuals present also with hypertension. In this context, the SPRINT trial showed that intensive control leads to a reduction in cardiovascular events both in frail persons,\(^{12}\) but this trial excludes most complex older adults, such as those presenting with cognitive impairment or psychiatric disorders, and those institutionalised. The lack of evidence regarding the treatment of hypertension in frail older people has been highlighted in the recently issued guidelines for the management of hypertension that recognise the role of BP-lowering therapy as one of the few interventions to reduce mortality risk in frail older individuals, but did not make any specific recommendations regarding treatment of hypertension in frailty individuals.\(^{14}\)
高血圧患者に対する RCT では、フレイルが除外基準になっています。しかし、フレイル患者の 70% が高血圧を有していることもわかったので、これは極めて重要な発見です。
Second, frailty is associated with limited life expectancy; as described by results of the SHARE study, life expectancy for frail individuals at age of 70 years ranges between 0.1 and 1.8 years in men and between 0.4 and 5.5 years in women.\(^{52}\) Therefore, in frail individuals the time-until-benefit of a given treatment might exceed the life expectancy and this might modify the risk–benefit ratio of preventive treatments for chronic diseases, including hypertension, which may require several years before showing a beneficial effect.
第2に、フレイルは、余命が短いという指摘もなされています。これも重要ですが、今回の研究で余命は出ていないので、唐突な印象を受けます。
Third, frail individuals have an increased risk of iatrogenic illness. Cullian et al showed among hospitalised older adults frailty doubles the risk of developing an adverse drug reaction.\(^{53}\) Finally, frailty might be associated with poor medication adherence to antihypertensive medications.\(^{54}\)
iatrogenic: 医師の診断から生じる、医原性の
さらに、入院患者の場合フレイルは薬剤の有害事象が倍になる、フレイルはアドヒアランスが低いといった結果に言及しています。
次の段落から、まとめに入っています。
These data underline the importance of assessing frailty when treating hypertension and possibly to set individual targets of BP control for persons with frailty. Interestingly, in the SPRINT trial frail participants in the intensive BP control group experienced a significantly lower reduction of SBP compared with non-frail participants (10.8 vs 13.5 mm Hg, p=0.01), underling possible difficulties in lowering BP in frail persons.\(^{12}\)
これらのデータは、高血圧の治療をする際にフレイル評価をすることの重要性を強調していると言えます。これまでの考察のまとめなので、詳細は省略します。
The meta-analysis of cross-sectional studies did not show any significant association between frailty and hypertension. Chronic diseases, including hypertension, are considered to be major determinants of frailty in theoretical models, and the negative effect of hypertension on cardiovascular outcomes can lead to frailty.\(^{55}\) However, our findings might be explained by the fact that cross-sectional data assess a single time point and are unable to evaluate the role of hypertension at differing stages of the frailty process.
Only four longitudinal studies assessed the impact of hypertension on incident frailty, providing conflicting results. This observation is in line with results of RCTs that were not able to show any impact of treatment of hypertension on onset of frailty.\(^{13 56}\) A possible explanation for this lack of effect could be that that persons developing frailty might be more likely to be lost to follow-up, and this selective drop out makes it difficult to draw any firm conclusions about the effect of the treatment on these frailty-related outcomes.\(^{57}\)
最後に、研究の強み (strength) と限界 (limitation) です。
Strengths and limitations
We performed a comprehensive literature search and a careful study selection and quality assessment, providing a reliable overview of the evidence in the field of hypertension and frailty. In addition, selected studies enrolled mainly community-dwelling samples and this enhances the generalisability of our findings. However, our findings present some limitations. First, we detected a significant heterogeneity among the studies which can be explained by the different definitions of frailty and hypertension and the demographic differences across studies. This heterogeneity is partially buffered by the absence of evident publication bias, and the reliability of our findings is increased by the low-to-moderate risk of methodological bias. Second, the cross-sectional design of 28 out of 32 studies limits the opportunity of assessing a cause–effect association between frailty and hypertension. In addition, the four longitudinal studies retrieved by our literature search provided conflicting evidence on the association between frailty and hypertension. Third, the meta-analyses included only studies that defined frailty based on the CHS criteria. Therefore, we cannot exclude that the described association of frailty with hypertension varies if different criteria for frailty definition are adopted. Finally, most of the studies included in the review were not aimed to assess hypertension and its relationship with frailty. For this reason, hypertension was poorly defined in most studies and this might lead to possible concerns about the methodology used to assess this condition.
研究の強みとしては、地域在住者がおおかったため、一般化可能性を強化しているとあります。15
15 external validity と同じ意味の英単語はどれか?
強みよりも限界の方が多くなっています。異質性が高かったこと、横断研究が多かったため因果関係を示すことができないこと、レビューした研究の目的が高血圧とフレイルの関係性を評価する目的ではなかったことなどがあります。
4.7 解答および解説
Q: What is the affiliation of the corresponding author?
A: Corresponding author は、
Correspondence to Dr Graziano Onder; graziano.onder@unicatt.it
とある。所属先 2 は、Università Cattolica del Sacro Cuore である。
Q. 英語以外の論文はすべて除外されたか?
組入基準が、
articles in English or another European language
なので、ヨーロッパ言語は除外されていない。
Q. バイアスリスクが低いとするのは NOS 何点か?
scores of <5 indicated high risk of bias.
<5 なので、4点以下。
Q. フルテキストを読んだ件数は何件か?
66 件。
Q: フレイルの定義として、Fried LP による CHS 基準以外に何があったか?
A: 該当する部分は、以下のとおり。
The rest of the studies evaluated frailty based on a frailty index (n=6),\(^{20 23 26 32 38 40}\) by a composite score (n=3)\(^{31 33 35}\) or using the Clinical Frailty Scale (n=1).\(^{48}\) One study assessed frailty adopting both CHS criteria and Frailty Index (FI).
フレイルの定義としては、Fraity Index、composit score、Clinical Frailty Scale の三種類が入った。なお、Frailty Index と CHS を使っているものもあった。
Q: 感度分析を行うにあたり、どのような研究に絞ってメタ分析を行なったか?
A: 該当する部分は、以下のとおり。
These results were confirmed when only studies with NOS ≥5 (OR 1.39; 95% CI 0.70 to 2.75; I\(^2\)=88.1%) or studies with a sample size ≥500 participants (OR 1.25; 95% CI 0.79 to 1.99; I\(^2\)=88.4%) were analysed.
Newcastle Ottawa Scale (NOS) が5以上の研究のみに絞っても、95% CI 0.70 から 2.75 なので有意差はなかった。
また、サンプルサイズが 500 以上の研究に絞っても、95% CI 0.79 から 1.99 なので有意差はなかった。
Q. external validity と同じ意味の英単語はどれか?
generalisability