8 Liu W (2020)
Saturday Morning RStudio 勉強会
毎週土曜朝6:30-9:00
8.1 論文
それでは、いよいよ横断研究の論文を読みましょう。
Liu W\(^1\), Puts M\(^2\), Jian F\(^3\), Zhou C\(^1\), Tang S\(^1\) and Chen S\(^4\) (2020) Physical frailty and its associated factors among elderly nursing home residents in China

- 中南大学湘雅护理学院, China1
- Lawrence S. Bloomburg Faculty of Nursing, U of Toronto, Canada
- 湖南師範大学医学院, China
- 九州大学
1 Corresponding author の所属先や ORCID は、サイト上のどこで確認できるか?
論文は、こちらにあります。
https://doi.org/10.1186/s12877-020-01695-5

Creative Commons Attribution 4.0 International License
8.2 用語
- prevalence は有病率のことですが、フレイルは病気ではないため、有症率やフレイル率などと訳されます。
患者は、住む場所に応じて3つに分類されます。タイトルから、これは “nursing home” であることがわかりますが、これは一般的には施設に該当します。なお、nursing home は、国による違いが大きく、高齢者専門ジャーナル JAMDA は、アメリカの nursing home は施設ではないとしています。この論文は中国の研究なので、施設で良いでしょう。
- community-dwelling patients 地域在住患者
- institutionalized patients 施設入所患者
- hospitalized patients 入院患者
comorbidity: 重複疾患
cut-off (points): スクリーニング検査等の基準値。カットオフ値。
8.3 Abstract
まず最初に Abstract を読みましょう。
Background Evidence is scarce on the trend in prevalence of physical frailty in China; the primary purpose of this study was to identify the prevalence and correlates of physical frailty among older nursing home residents in China.
- 中国の施設在住高齢者のフレイル率はまだエビデンスがない
Methods Cross-sectional study in 20 nursing homes in Changsha, China. Physical frailty was defined based on the frailty phenotype including weight loss, low grip strength, exhaustion, slow gait speed, and low physical activity. Participants with at least three affected criteria were defined as being frail. Participants with one or two affected criteria were considered as pre-frail, and those with no affected criteria were considered as robust. A total of 1004 nursing home residents aged 60 and over were included in this study. A multinomial logistic regression model was used to analyze the associations of physical frailty with its potential risk factors, including age, sex, education levels, marital status, type of institution, living status, current drinking, current smoking, regular exercise, and self-reported health.
- 中国の長沙市の20の老人ホームで調査
- 老人ホーム在住者で60歳以上の1004名
- 多項ロジスティック回帰で関連因子を調査
Results The overall prevalence of physical frailty and prefrailty was 55.6, and 38.5%, respectively. The rate of physical frailty substantially increased with age, and was higher in women than in men (69.5% vs. 30.5%). The multinomial logistic regression analysis showed that older age, being women, living in a private institution, living alone or with unknown person, having no regular exercise (≤ 2 times/week), and poor self-reported health were significantly associated with increased odds of being physically frail.
- フレイル率は55.6%、プレフレイル率は38.5%
- フレイルは、年齢、性別、私立老人ホーム、一人暮らし、運動習慣、自己報告不健康と関連
Conclusion We demonstrated physical frailty is highly prevalent among older residents in nursing homes in China, especially in women. The potential role of those associated factors of physical frailty warrant further investigations to explore their clinical application among elderly nursing home residents.
- 中国の施設在住高齢者のフレイル率は高いことがわかった。
以上で、Abstract は終わりになります。通常、ロジスティック回帰の Abstract では、説明変数のオッズ比も掲載されることが多いですが、ここは掲載されていません。
では、ロジスティック回帰とはどういう解析を行うのでしょうか?Abstract によると、「多項」ロジスティック回帰とあります。これはなんでしょうか?これらは Methods で解説します。
8.4 Background
There is a growing research interest in frailty worldwide, especially in countries where the population is rapidly aging, including China [1, 2]. Frailty refers to a state of increased vulnerability to stressors, characterized by a decreased physiological reserves [3, 4], resulting in an elevated risk of adverse health outcomes, such as falls, disability, hospitalization, delirium and mortality [5, 6]. Although there is no universal consensus in the operational criteria used in different practice settings and epidemiological investigations [7], two main operational approaches have been widely used to measure frailty: the frailty phenotype [5] and the Frailty Index [8]. The Frailty Index is composed of at least 30 Items and can be obtained through a comprehensive geriatric assessment [3]. The frailty phenotype can be calculated by having older adults complete simple tasks without a preliminary clinical evaluation. The frailty phenotype is more easily identified objectively in older nursing homes residents who are at increased risk of negative events [9]. However, due to the differences (i.e., physiological and psychological dimension) in different populations, there are no reference criteria for the frailty phenotype in older adults living in nursing homes in China.
本文の最初は Background です。まずは、背景をまとめてみましょう。
… Frailty refers to a state of increased vulnerability to stressors, characterized by a decreased physiological reserves …
increased vulnerability や、decreased physiological reserves はとても訳しづらい英語です。ただ、フレイル論文では定番のような表現でもあります。定番なので、多くの訳もあります。おおむね、このように訳されています。「フレイルとは、ストレスに対する脆弱性が亢進した状態で、生理的予備能が低下する特徴がある。」
… two main operational approaches have been widely used to measure frailty: the frailty phenotype [5] and the Frailty Index [8]. 2
2 Frailty Index は、何項目からなる判定方法か?
フレイルの操作定義の方法としては、表現型と Frailty Index という二つの方法がある、とされています。
実は、読み進めてみるとわかりますが、この研究のフレイルの判定方法は Fried LP の Phenotype 法です。ここでわざわざ Frailty Index を紹介する意図はわかりかねます。
- No reference criteria for the frailty phenotype in older adults living in nursing homes in China
先行研究では、「西洋の施設在住高齢者」や「中国の地域在住高齢者」のフレイル率は報告されています。
According to various previous studies among community-dwelling older adults in Western countries, the prevalence of frailty varied enormously (range 4.0 to 59.1%), which is likely due to different measurement tools and frailty definitions used [10].3 The prevalence of frailty has been reported to vary between 5.9 to 17.4% in China [11].
3 先行研究によると、地域在住の高齢者のフレイル率は何%から何%か?
10 Collard RM, Boter H, Schoevers RA, Oude Voshaar RC. Prevalence of frailty in community-dwelling older persons: a systematic review. J Am Geriatr Soc. 2012;60(8):1487–92.
11 He B, Ma Y, Wang C, Jiang M, Geng C, Chang X, Ma B, Han L. Prevalence and risk factors for frailty among community-dwelling older people in China: a systematic review and meta-analysis. J Nutr Health Aging. 2019;23(5):442–50.
第2段落の最後に、この論文の目的が記述されています。
According to various previous studies among community-dwelling older adults in Western countries, the prevalence of frailty varied enormously (range 4.0 to 59.1%), which is likely due to different measurement tools and frailty definitions used [10]. The prevalence of frailty has been reported to vary between 5.9 to 17.4% in China [11]. For residents living in nursing homes, physical frailty is highly prevalent (range 19.0 to 75.6%) in western populations [12]. Numerous studies on frailty in China, to date, have been conducted in community-dwelling older adults [11], but epidemiological data is scant among older nursing home residents [13]. Compared to community-dwelling older adults, individuals living in nursing homes might be more vulnerable and tend to simultaneously have multiple risk factors of frailty (i.e., self-reported health status, activity of daily living disability) [14,15,16]; consequently, the prevention and management of frailty could be more challenging in nursing homes. Therefore, it is of substantial clinical interest to identify the prevalence of physical frailty and its modifiable risk factors among elderly nursing home residents. Such epidemiological evidence could help to develop effective interventions for the prevention and management of physical frailty in the nursing homes setting to delay the onset of frailty and maintain independence in daily activities [17,18,19]. Thus, in this present study, we aimed to investigate the prevalence of physical frailty and its associated factors among older people living in nursing homes in China.
研究の目的を示すときの表現
- The purposes of this study were to …
- We aimed to …
… we aimed to investigate the prevalence of physical frailty and its associated factors among older people living in nursing homes in China.4
4 本研究の目的は何か?
prevalence of physical frailty は、老人ホームにおける調査時点でのフレイルの有病率です。
associated factors は、関連する因子です。これは通常ロジスティック回帰で求め、結果はオッズ比で示されます。
8.5 Methods
Methods では、研究の方法が書かれています。
Study design and participants
This cross-sectional study was conducted between January 2018 and April 2019 and involved 20 nursing homes in the metropolitan area of Changsha, China. A total of 2630 adults, aged ≥60, were invited to participate in this study. Changsha is a middle-size provincial city with a population of 8 million in the central region of China, which has the characteristics of low population mobility and a traditional Chinese lifestyle [20]. The survey comprised questionnaires, anthropometric measurements, and physical fitness tests, which were conducted according to the standard protocols of the study assessment tools. The questionnaire survey was completed via face-to-face interviews by well-trained nurses. In this study, inclusion criteria were as follows: having clear consciousness identified by registered nurses in nursing homes and the ability to communicate independently, including people who were visually or hearing impaired but could communicate through family members as identified by nursing home staff in each of the homes. We contacted all eligible participants by sending brochures explaining the study and inviting them to participate (n = 2550), and a total of 2204 residents agreed to participate in the survey, with a response rate of 86.4%. Of those, 1607 participants who completed the baseline survey by sending brochures were included in this study (597 died or moved out of those nursing homes during the survey period). We excluded participants who had a history of dementia (n = 66), Parkinson’s disease (n = 52), stroke (n = 208), or a Mini-Mental State Examination (MMSE) score < 18 (n = 69). Also, participants with missing data on any components of physical frailty were excluded (n = 208). Therefore, the final sample included 1004 participants (339 men and 665 women) (Fig. 1).
- cross-sectional study5
- 20 nursing homes, 2630 adults
5 研究デザインは何か?
この研究は、観察研究のうち、コホート横断研究です。
後半 (We contacted all eligible participants by sending brochures explaining the study and inviting them to participate (n = 2550),) は、通常は Results に書かれる内容
次の段落では、Fried のフレイル基準を詳しく解説しています。
Physical frailty
Frailty was defined according to the phenotype of physical frailty [5], which consists of weakness, slowness, low level of physical activity, shrinking and exhaustion [5]. The operational definitions of each component are shown in Table 1. Weakness was measured in kilograms by a handgrip dynamometer (KD - WLJ; KonDak, China). Participants were required to perform the test twice for each hand in a standing position. The maximum value among the four measurements was used for the analyses. The cut-off points [21] were stratified by sex and body mass index (BMI). Slowness was defined as the average walk speed in a 5-m walking test. Starting from a motionless position, participants were instructed to take this test twice, and the time (seconds) of gait speed was recorded with a digital stopwatch between the 3 and 8 m in each trial. We measured the time taken (in seconds) to pass 8 m to calculate gait speed (m/s). The cut-off points [21] were slow gait speed as stratified by sex and standing height. We used the cut-off points [21] in weakness and slowness referring to the general older adults in the CHARLS cohort, which was previously conducted and validated by the population-based lowest quintile [5]. Low level of physical activity was measured with the Chinese version of the Physical Activity Scale for the Elderly (PASE) questionnaire [22]. The cut-off points were stratified by sex to collect physical activity scale data [23]. Shrinking was measured by unintentional weight loss > 5 kg during the previous year, except for dieting or exercise. Exhaustion was determined on the basis of a positive answer to either of the following two self-reported questions of the Center for Epidemiologic Studies-Depression (CES-D) Scale [24]: “I felt that everything I did was an effort” (in the past month) and “I could not get going.” According to the frailty phenotype [5], participants with three or more affected components were considered frail, those with one or two affected components were considered prefrail, and those without any component were considered robust.
Fried のフレイルの基準についてよくまとまっています。
6 歩行速度はどのように計測したか?
7 Shrinking とは何か?
Slowness was defined as the average walk speed in a 5-m walking test. Starting from a motionless position, participants were instructed to take this test twice, and the time (seconds) of gait speed was recorded with a digital stopwatch between the 3 and 8 m in each trial. We measured the time taken (in seconds) to pass 8 m to calculate gait speed (m/s).
高齢者の歩行速度は、8 m 以上歩いていただき、その中間の 3 m から 5 m の間の速度を計測しました。
Shrinking was measured by unintentional weight loss > 5 kg during the previous year, except for dieting or exercise.
意図しない体重減少が 5 kg より多いかという項目です。
通常、成人は体重増加が問題になっていますが、高齢者になると体重減少の方が問題となります。
Correlates of physical frailty
Information on the following covariates was collected through the questionnaire: age, sex, education level (elementary and below, or junior middle school and above), marital status (married, other [widowed, divorced, never married]), type of institution (public or private), living status (living with husband/wife, living with alone or others [unknown person]), current drinking (yes or no), current smoking (yes or no), regular exercise (≤ 2 times/week, ≥ 3 times/week), and self-reported health (very good or good, fair or poor). Basic activities of daily living (ADL), as the correlate of frailty, was measured by the Katz scale, which comprises including the following 6 items: bathing, dressing, toileting, transferring, continence, and feeding [25]. Disability in ADL ability was defined as having difficulty and/or requiring assistance in time ≥ 1 activities. Information on the medical history of diseases was collected from the medical records by physicians. Comorbidity was defined as having 2 or more of the following 9 diseases, hypertension, diabetes, cancer, chronic heart disease, stroke, chronic digestive disease, arthritis/rheumatism, chronic lung disease, and chronic kidney disease.
ロジスティック回帰では、共変量は複数設定することができます。ここでは、
- 年齢、性別、教育歴、婚姻状態
- type of institution8
- 現在の飲酒、喫煙
- 運動習慣
- 自己報告の健康状態
- ADL (Katz scale)
- 重複疾患 (comorbidity)
8 Institution とは何か?
Statistical analysis
The characteristics of the sample were summarized according to physical frailty groups. Categorical variables were presented as percentages. Trends in characteristics across physical frailty status were tested using the Cochran-Mantel-Haenszel test. Odds ratios (OR) with 95% confidence interval (CI) of physical frailty for the potential associated factors were estimated by using multinomial logistic regression models. The logistic regression model included age (continuous), women (reference men), low education level (reference junior middle school and above), being widowed or divorced or never married (reference being married), living in a private institution (reference public), living alone or with unknown person (reference living with husband/wife), current drinking (reference no), current smoking (reference no), regular exercise ≤2 times/week (reference regular exercise ≥3 times/week), and poor self-reported health (reference very good/good self-reported health). A Venn diagram was used to illustrate the overlap of ADL disability and comorbidity with physical frailty.
All statistical analyses were performed using IBM SPSS Statistics Version 24.0 (IBM; Armonk, NY, USA). All p-values were two-tailed, and p ≤ .05 was considered statistically significant.
統計について書かれているところを読んでみましょう。
… Odds ratios (OR) with 95% confidence interval (CI) of physical frailty for the potential associated factors were estimated by using multinomial logistic regression models.9 …
9 なぜロジスティック回帰ではなく多項ロジスティック回帰を用いたか?
ここにあるように、多項ロジスティック回帰を用いてオッズ比を推定しています。
ロジスティック回帰 (logistic regression) とは、
type of regression model used to analyze the relationship between a binary dependent variable and 1 or more independent variables.
ここでのポイントは、アウトカム (上の記述では従属変数 dependent variable) は、二値変数 (binary) とあります。つまり、「生または死」「発症または未発症」など、二つの値だけを取ります。
多項ロジスティック回帰 (multinomial logistic regression) は、二値変数を三値以上に拡張したものです。
フレイルの場合、「発症または未発症」ではなく、「フレイル、プレフレイル、頑健」の3つに分類されることが多いため、多項ロジスティック回帰を使われることが多くなります。
… The logistic regression model included age (continuous), women (reference men), low education level (reference junior middle school and above), being widowed or divorced or never married (reference being married), living in a private institution (reference public), living alone or with unknown person (reference living with husband/wife), current drinking (reference no), current smoking (reference no), regular exercise ≤2 times/week (reference regular exercise ≥3 times/week), and poor self-reported health (reference very good/good self-reported health).10 …
10 共変量は、…
共変量は、前の節と同じ内容が列挙されています。ただし、ここでは連続数値なのかどうか、カテゴリ変数の場合は、どれを参照としたかが書かれています。例えば、
- age (continuous): これは、連続数値として扱っています。 数値の場合、結果は数値が 1 上昇する際のアウトカムのオッズ比が示されます。
- women (reference men): この場合、男性を参照 (reference) として女性のオッズ比を求めます。
8.6 Results
結果を見てみましょう。まず、参加者背景とフレイル率についてみてみます。
Participants were 60 to 107 years of age, with mean age of 80.8 (standard deviation [SD] 8.9) years and 33.8% were men. The prevalence of physical frailty and prefrailty were 55.6 and 38.5% respectively. In men, 37.2% were pre-frail and 30.5% were frail; in women, 62.8% were pre-frail and 69.5% were frail. Table 2 shows characteristics of participants according to physical frailty status. A trend test of all factors across physical frailty status revealed that those participants who were more frail compared with participants who were less frail, tended to be older, more likely to be women, to be widowed or divorced or never married, to be living in a private institution, to be living with alone or others (unknown person), to report poor health status, and were less likely to have regular exercise.
Participants were 60 to 107 years of age, with mean age of 80.8 (standard deviation [SD] 8.9) years and 33.8% were men. The prevalence of physical frailty and prefrailty were 55.6 and 38.5% respectively.
平均80.8歳 (SD 8.9)、33.8% が男性です。フレイル率は 55.6%、プレフレイルは 38.5% という結果となりました。
respectively は、「それぞれ」の意味で、数値を多く列挙する場合によく使われます。
Table 2 shows characteristics of participants according to physical frailty status.11
11 Table 2 から、有意差が見られるのはどの項目か?
Figure 2 shows the prevalence of physical frailty by sex and age group. The prevalence of physical frailty increased with each successive 5-year age group (p for trend < 0.001). The increasing trend of the curve was similar in both men and women. The percentage of physical frailty dramatically increased from the 75–79 age group, especially in women.
Figure 2 shows the prevalence of physical frailty by sex and age group. The prevalence of physical frailty increased with each successive 5-year age group (p for trend < 0.001). The increasing trend of the curve was similar in both men and women. The percentage of physical frailty dramatically increased from the 75–79 age group, especially in women.
Figure 3
Figure 3 shows the results of multinomial logistic regression model on the associations of physical frailty with its potential risk factors. The multivariable-adjusted OR with each five-year increment in age was 2.20 (95% CI 1.79–2.70) for being frail and 1.73 (95% CI 1.41–2.11) for being prefrail compared to the robust group. Women were approximately 5 times more likely to be frail (multivariable-adjusted OR 4.98, 95% CI 2.41–10.28), and 3.5 times more likely to be prefrail (multivariable-adjusted OR 3.48, 95% CI 1.69–7.15) than men. Living alone or others (unknown person) was associated with significantly increased odds of frailty (multivariable-adjusted OR 5.49, 95% CI 3.00–10.05) and prefrailty (multivariable-adjusted OR 3.12, 95% CI 1.25–7.76). Compared with participants with regular exercise, those who were not engaged in regular exercise had a fourfold higher risk of being frail (multivariable-adjusted OR 4.46, 95% CI 1.84–10.84) and a twofold higher risk of being prefrail (multivariable-adjusted OR 2.49, 95% CI 1.03–6.01). Those who reported poorer self-reported health were approximately 4 times more likely to be frail (multivariable-adjusted OR 3.77, 95% CI 1.82–7.80) and 2 times more likely to be pre-frail (multivariable-adjusted OR 2.07, 95% CI 1.03–4.16). Living in private (vs. public) institutions was associated with increased odds of frailty (multivariable-adjusted OR 2.96, 95% CI 1.42–6.19), but not with prefrailty. No statistically significant associations were found between frailty status and education level, marital status, current drinking and current smoking.
Women were approximately 5 times more likely to be frail (multivariable-adjusted OR 4.98, 95% CI 2.41–10.28), and 3.5 times more likely to be prefrail (multivariable-adjusted OR 3.48, 95% CI 1.69–7.15) than men.12
12 アクティブラーニング課題: “Women were approximately 5 times more likely to be frail (multivariable-adjusted OR 4.98, 95% CI 2.41–10.28)” という表現は正しいか?
comorbidity: 重複疾患
Figure 4 は、フレイルと ADL 障害と重複疾患の重なりを示しています。
前提として、Fried LP (2001) に同様の図がありました。
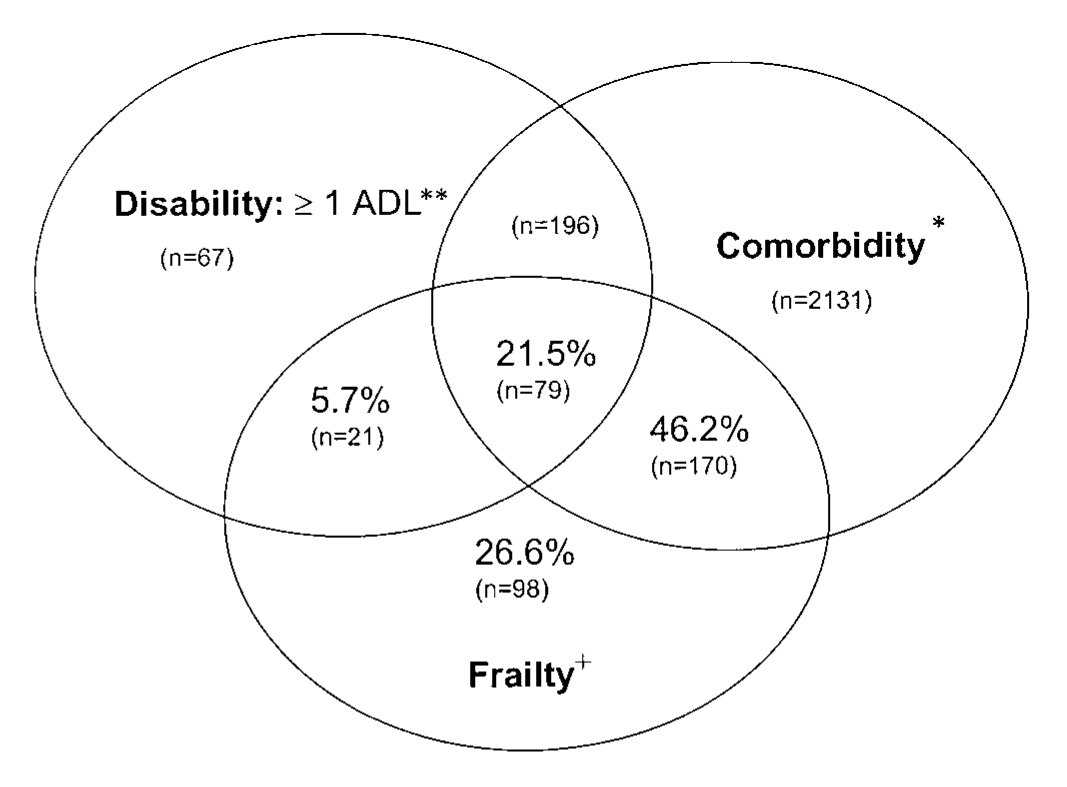

Figure 4 shows the overlap of ADL disability and comorbidity with frailty. Among the overall 1004 participants, each participant had at least one of those three conditions. Of these who were frail, 12.7% had comorbid diseases, 8.0% had ADL disability, 32.2% had both comorbid disease and ADL disability, and 2.7% had neither ADL disability nor comorbidity.
Figure 4 shows the overlap of ADL disability and comorbidity with frailty. Among the overall 1004 participants, each participant had at least one of those three conditions. Of these who were frail, 12.7% had comorbid diseases, 8.0% had ADL disability, 32.2% had both comorbid disease and ADL disability, and 2.7% had neither ADL disability nor comorbidity. 13
13 以下は、Fig 4 を読み取っている文章であるが数値が間違っている。どのように間違っているか?
Of [those] {who were frail},
注: 原文では these となっているが、those が正しい。
関係代名詞 who と「人々」を表す先行詞 those を使っている。「{フレイルである}[人々]のうち」
neither A nor B: A も B も~ではない
8.7 Discussion
In this present study, our results showed that physical frailty was highly prevalent among older adults living in nursing homes in China, especially in women. We observed older age, being women, living in a private institution, living alone or others (unknown person), having no regular exercise, and poor self-reported health was significantly associated with physical frailty. Also, we found that although physical frailty, to some extent, overlapped with disability and comorbidity, many frail participants did not have disability or comorbidity, suggesting that physical frailty did not equate with comorbidity or disability in this study’s population of nursing home residents. At present, there is no the gold standard for comprehensive geriatric assessment as part of the admissions procedure to nursing homes in China. Most nursing in homes in North America and Europe use the Resident Assessment Instrument (RAI), data from which corresponds directly to the frailty index [26], however, such the RAI is currently not utilized in China.
physical frailty was highly prevalent among older adults living in nursing homes in China
中国では、老人ホーム居住者のフレイル率が高いことが示されました。
Significantly associated with physical frailty:
- older age,
- being women,
- living in a private institution,
- living alone or others (unknown person),
- having no regular exercise, and
- poor self-reported health
これは、ロジスティック回帰によって有意差があるとされた共変量です。
many frail participants did not have disability or comorbidity
フレイル参加者の多くは、障害や重複疾患を持っていなかった。14
14 この文章にはおかしな点がある。図を参照しておかしな点を説明しなさい。
Most nursing in homes in North America and Europe use [the Resident Assessment Instrument (RAI)], {data from which corresponds directly to the frailty index}, however, such the RAI is currently not utilized in China.
関係代名詞と前置詞の組み合わせです。関係代名詞節の部分を { } 、先行詞を [ ] で示しています。
北米とヨーロッパのほとんどの老人ホームは [ RAI ] を使用している。
{ [ RAI ] からのデータは Frainty Index に直接対応している。 }
しかしながら、RAI のようなものは中国では使われていない。
“nursing in homes” の “in” はおそらく不要。however を接続詞のように使っていますが、おそらく but の方が正しい。
第2段落は、第1段落を詳しくしただけのものなので、省略します。
第3段落は、性差について考察しています。15
15 Question 4.2 筆者らは、なぜ女性の方がフレイルが多いと考えているか。
In agreement with some previous studies from other countries [10, 21, 32], we also observed that the prevalence of frailty increased with older age. In terms of the associations between physical frailty and status of the institution (private versus public), the present study was the first, to our knowledge, in which such an association was observed. One possible explanation could be that older adults living in private institutions (more expensive in the metropolitan areas than public institutions) usually have higher social economic status, are perhaps more likely to feel more lonely [13] and suffer loss of appetite [33] when staying away from family and changing their ways of previous life, resulting in higher likelihood of being frailer. Compared with people living with their partners in the same nursing home, those who live with alone or share the room with unknown person may become more frail because of poorer social ties [34] and mental disorders [35]. In line with previous studies [36, 37], we also found that regular exercise was associated with physical frailty. One explanation is that there is a vicious cycle: due to the fear of falling [38], as the level of frailty increases, so does the tendency to avoid taking regular exercise. Participants with frailty had poorer self-reported health in our study, in concordance with results from previous studies [14, 39, 40]. This might be explained by the fact that frail older people have a state of greater vulnerability [41], so they were more likely to rate their health poorly. In all, the potential role of those factors of physical frailty warrant further investigations to explore their clinical application among elderly nursing home residents.
adiposity: 脂肪症、肥満性
理由については、3点挙げています。
… Abdominal adiposity was associated with systemic inflammation by mediating its link with metabolic syndromes, which were important markers of oxidative stress and result in skeletal muscle damage and low grip strength [30]. …
まず、引用文献 [30] を使い、腹部の脂肪によって炎症を起こしている可能性を示しています。
In our study of nursing homes in China, on average female residents were older than male residents and were better able to take care of themselves and others and to arrange their care. …
次に、女性の方が年齢が高かった点を挙げています。つまり、共変量同士に関連があった可能性があります。
It could be that men are admitted with lower frailty levels when they live alone because they are less able to support or organize support for themselves [31].
さらに、引用文献 [31] を使い、男性は一人では生活できないため、フレイルレベルが低くても施設に入所するとしています。
Reduced physical function reserve (i.e., physical frailty) may occur without showing any difficulties in tasks of daily living or having multiple chronic diseases [5]. However, there are concerns as to whether physical frailty is synonymous to disability or comorbidity among older adults in nursing homes in China. This is because most older adults who moved to nursing homes are usually severely physically dependent and suffering from comorbidities [42,43,44] as older people usually live at home with their families, in keeping with the traditional Chinese family values [45, 46]. In the present study, in contrast, we found that many frail participants did not have disability or comorbidity, indicating that physical frailty did not equate with comorbidity or disability in the population of elderly nursing home residents. Our findings suggest that, physical frailty, related but distinct from disability and comorbidity, can be integrated into nursing-home settings as part of risk stratification and may serve a useful target for preventive interventions.
Question 4.3: アクティブラーニング課題 老人ホームの種類や配偶者と入所している点について、日本ではどうだと考えられるか?
synonymous: 同義語
there are concerns as to whether physical frailty is synonymous to disability or comorbidity among older adults in nursing homes in China.16
16 結果でも見たように、この部分は誤っている。よって、この後の考察もおかしなものとなっている。
Our findings suggest that, physical frailty, related but distinct from disability and comorbidity, can be integrated into nursing-home settings as part of risk stratification and may serve a useful target for preventive interventions.
研究の強み (strengths)
Our study had several strengths. Firstly, weakness and slowness for defining physical frailty were recorded using objective measures. Secondly, this study comprehensively reports examined substantial sociodemographic differences in physical frailty prevalence. However, there were limitations to our study. Firstly, due to the cross-sectional study design, there was no follow up to observe the progression from pre-frailty to frailty, and we could not establish causality of frailty and adverse health outcomes. Therefore, further research will be needed to verify the temporality of the exposure-effect association. Secondly, because of the relatively low response rate, there is a possibility of selection bias might have existed in our study. We could speculate that the nursing home residents who did not participate may be frailer. Thirdly, participants in our study were recruited from in one city, which is a capital city in the central region of China with a specific regional representation having low population mobility and a conventional Chinese lifestyle; therefore, caution should be practiced to generalize the findings of our study applicable to the whole of China. Finally, because most older adults in nursing homes were mostly 80 years and over, we might have underestimated frailty status.
- 筋力と速度は客観的
- 社会人口学的項目を包括 (comprehensive)
限界 (limitations)17
17 研究の限界 (limitations) について妥当だと考えるか?
- 横断研究であり追跡できていない
- 回収率が低いため、バイアスの可能性がある
- 1年のみであり一般化できない
8.8 Conclusion
結論
- フレイルは中国の老人ホームで多く見られた
- 関連因子は、年齢、女性、私立老人ホーム、一人暮らし、運動習慣なし、自己報告で不健康
- フレイルは改善可能なため、老人ホーム患者も予防的介入の対象となる
8.9 解答および解説
通常、ロジスティック回帰分析では、目的変数は2値変数でなければならない。しかし、この研究は robust、prefrail、frail の3値変数であるため、多項ロジスティック回帰分析を用いた。
有意差は、 p < 0.05 のもの。すなわち、
- 年齢
- 性別
- 婚姻状態
- 施設種別
- 配偶者と一緒に入所しているか
- 運動習慣
- 自己報告の(不)健康感
医学論文では、リスク比、ハザード比、オッズ比などの「比」がよく出てくる。リスク費やハザード比は 5.0 であれば「5倍なりやすい」と言える。オッズ比は必ずしもこうは言えない。
図中の数値は、全体(フレイル患者+非フレイル患者)に占める割合。フレイル患者(左下の円)に着目すると、
- comorbidity = (128+323)/(27+128+323+80) = 80.8%
- ADL disability = (80+323)/(27+128+323+80) = 72.2%
- 両方 = (323)/(27+128+323+80) = 59.9%
- neither = (27)/(27+128+323+80) = 4.9%
研究の限界には、3点 (横断研究であり追跡できていない、回収率が低くバイアスの可能性がある、1年のみであり一般化できない) あった。このうち第1点と第3点は、研究計画段階でわかっていたことであり、それほど重要ではない。一方、回収率が低かった点については、バイアスの可能性を報告している妥当な記述である。
8.10 アクティブラーニング課題
- Changsha とはどう言う街か?
- Figure 2 と Figure 3 を英文で読み取り、英文で記述しなさい (前者は 100 words 程度、後者は 250 words 程度)。